Introduction
Sodium-taurocholate Co-transporting Polypeptide (NTCP) is a member of the solute carrier membrane transport proteins. It is found within the membrane of
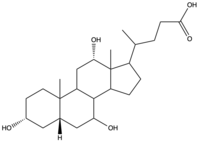
Figure 1. Structure of Cholic Acid, an example of a bile acid.
, and its primary role is to facilitate the transport of
bile salts into hepatocytes from the bloodstream (Fig. 1).
[1] This is important because 90% of human bile salts are recycled daily, so the function of NTCP is critical in providing bile acids to solubilize fats for digestion. In addition to transporting bile acids into the cytoplasm of hepatocytes, NTCP also serves as a receptor for
Hepatitis B (HBV) and
Hepatitis D (HDV) viruses.
[2] 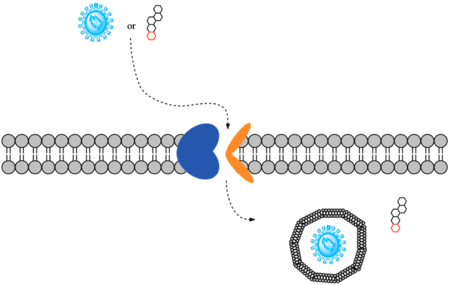
Figure 2. Overall mechanism of NTCP.
Structure
NTCP is a transmembrane protein found in hepatocyte cells. It consists of nine , with the N-terminus located on the extracellular side of the plasma membrane and the C-terminus located on the intracellular side (Figure 3). Transmembrane helices are connected by short loops as well as extracellular and intracellular alpha helices that lie nearly parallel to the membrane.[2] Structures were determined by cryogenic electron microscopy (Cryo-EM) of NTCP in complex with antibodies or nanobodies. [1] [2] [3] [4]
Domains
NTCP contains : the core and panel domains. Movement of these two domains allows recognition and transport of bile acids into hepatocytes.
- Panel Domain:
- Formed by transmembrane helices TM1, TM5, and TM6.
- Core domain:
- Formed by the packing of a helix bundle of TM2, TM3, and TM4 with another helix bundle of TM7, TM8, and TM9. These two helix bundles are related by pseudo two-fold symmetry.[5]
Proline/Glycine Hinge
in the connecting loops and extra- and intracellular helices (Figure 3) act as hinges in the mechanism of bile salt uptake. This flexibility allows separation of the core and panel domains, creating a pore open to the extracellular space and exposing critical Na+ binding sites. Once substrate binds the open-pore state, this hinge allows the transition to close this pore relative to the extracellular side and open to the cytoplasmic side, thus allowing release of substrate into the cell.[1]
Sodium Binding Sites
To transport a single bile salt from the blood to the cytoplasm of the hepatocyte, two sodium ions are required to be bound to to NTCP in the open-pore state.[4] Thus, there are two . The residues in the include Ser105, Asn106, Thr123, and Glu257. The residues in the include Gln68 and Gln261. Mutations to these significant residues inhibit the binding of sodium ions, and consequently, inhibit the transport of bile salts by NTCP.[4] Secondary active transport is used here, as the transport of bile acids into the cell is so thermodynamically unfavorable that the reaction has to be coupled to the favorable transport of two sodium into into the cell.[1] . When the bile salts are released into the cell, the protein is then found in the inward facing conformation, in which the pore through which the it had just passed is now closed to the extracellular side.
Significant Residues for HBV/HDV Infection
The majority of residues involved in bile salt uptake are also involved in HBV/HDV infection. (extracellular view) of Human NTCP have been shown to be vital for HBV/HDV virus recognition along with bile salt uptake. These residues were replaced in mice NTCP by human NTCP and conferred to successful binding of the virus. These residues are found in the extracellular loop connecting TM2 and TM3.[3] (extracellular view) have also been shown to be vital for HBV/HDV viral recognition and bile salt uptake. These residues were mutated in monkey NTCP to the human residues and preS1 binding was then successful. These residues are found on the N-terminal end of TM5. The absence of residues in either of these hinders preS1 binding and therefore HBV/HDV infection. Interestingly, residues 84-87 do not affect bile acid uptake, so it is a potential site for blocking HBV/HDV infection while maintaining NTCP's ability to perform its normal function.[3] Another important residue was discovered to be a single-nucleotide polymorphism in a small population in East Asia. , which is normally serine, being mutated to phenylalanine prevents preS1 binding and does not support bile acid transport. This residue is also found extracellularly, on TM8 of NTCP.[5] There are 3 additional leucine residues that when mutated, block both preS1 binding and HBV/HDV infection. Replacing with tryptophan residues presumably blocks the preS1 binding site preventing proper infection.[3]
Function
Mechanism of Bile Salt Uptake
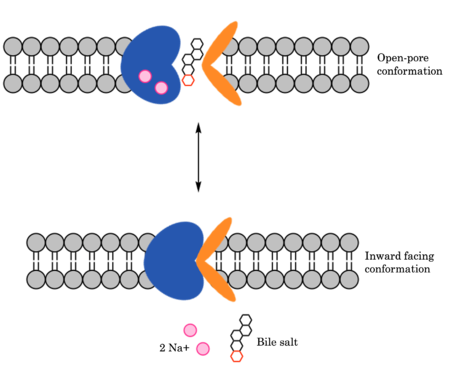
Figure 4. Mechanism of Bile Salt Uptake by NTCP.
NTCP utilizes secondary active transport to uptake bile salts from blood into the cytoplasm of liver cells (Figure 4). NTCP is crucial for bile salt homeostasis. Specific substrate binding pockets for bile salts have not been identified on NTCP, so the exact mechanism of uptake is unknown. However, it is known that bile salts recognize and bind to the , characterized by an exposed region on the extracellular side. After binding, bile salts pass through the amphipathic pore (INSERT GREEN LINK), and NTCP transitions into the . In this conformation, the pore closes off relative to the extracellular side and opens to the cytoplasmic side. Transition to the inward facing state allows release of bile salts and sodium ions. It is not yet known how this transition exactly proceeds.[2]
Mechanism of HBV/HDV Infection
HBV and HDV viruses are transported through NTCP via secondary active transport. After binding to NTCP in the , the viruses remain bound until low bile salt levels in the blood shift equilibria enough that endocytosis of the virus occurs. Once inside the cell, the viral genetic information is released and infection begins. The exact mechanism of how HBV and HDV bind to NTCP is not certain, although have been identified on NTCP: residues and .[3] An additional single-nucleotide polymorphism was discovered in East Asia involving being mutated from serine to phenylalanine. This mutation prevented HBV/HDV infection. Another mutation, replacing with tryptophan presumably blocks the preS1 binding site preventing proper HBV/HDV infection.[3] It has also been shown that myristoylation of the HBV/HDV capsid is vital for recognition by NTCP, as well as residues 8-17 on HBV/HDV (sequence: NPLGFFPDHQ). There are two proposed mechanisms for how HBV/HDV binds to NTCP. The first proposes binding of the myristoyl group to the host cell membrane, while residues 8-17 interact with NTCP residues 157-165. The second proposes binding of the myristoyl group with residues 157-165 in the pore.[6]
Medical Relevance
Bile salts are derived from cholesterol, and they serve an important role in the mechanical digestion of fats and ultimately facilitate the chemical digestion of lipids. The amphipathicity allows them to do this, solubilizing hydrophobic fats for transport in aqueous bodily fluids. Without bile salts, fats would spontaneously separate out of the aqueous solution in the duodenum and would not be accessible pancreatic lipase for breakdown. Proper fat digestion requires both pancreatic lipase and bile; thus, NTCP's function in recycling bile salts is critical.[7]
Insight into NTCP's structure and function has implications for therapeutic treatment of HBV/HDV infection. For example, the inhibitory effect of Nb87 on myr-preS1 binding shows potential for therapeutics that stabilize NTCP inward-facing state as allosteric inhibitors of viral cell entry. [6]
Additionally, bile acids play a major role in the regulation of lipid and energy metabolism, so research conducted on mice concluded that targeting NTCP-mediated bile acid uptake can be an innovative way to treat obesity and obesity-related hepatosteatosis through the simultaneous dampening of intestinal fat absorption and increasing energy expenditure.[8]




